

1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Cervical Spine Mobilization program
2.3. Cervical stabilization movement program
2.4. Stretching exercise program
2.5. Mesurements
2.6. Statistical analysis
3. Results
3.1. Subjects
3.2. Changes in the range of neck joint movement
3.3. Change in muscle functions
3.4. Changes in the neck pain VAS and NDI
4. Discussion
5. Conclusion
1. Introduction
With the widespread use of internet-connected devices, technology plays a crucial role in our daily livings. While it confers substantial benefits particularly in communication and productivity, it also brings health concerns. Prolonged use of smartphones and computers can lead to poor posture and ergonomic strain, often causing musculoskeletal pain. Recently, young people report neck, shoulder, and thumb pain linked to mobile device uses (Mekhora, Liston, Nanthavanij, & Cole, 2000). These repetitive and unfavorable physical conditions can lead to chronic non-specific neck pain.
Chronic non-specific neck pain, defined as lasting over 12 weeks, lacks clear pathological signs or diagnostic markers (Childs et al., 2008). It typically affects the upper cervical spine without structural damage such as fractures or infections (Hidalgo et al., 2017). It’s the second most common pain condition after back pain and is costly to manage (McLean, May, Klaber-Moffett, Sharp, & Gardiner, 2010). The global prevalence is approximately 0.8%, with higher rates observed in women and older adults (Safiri et al., 2020).
Though often linked to poor posture, muscle imbalance, or tension, the pathophysiological mechanisms remain unclear (Cheng et al., 2014). Symptoms include limited mobility and muscle dysfunction, which are associated with the central nervous system (Treleaven, 2008).
Non-specific neck pain is typically treated with non-invasive methods like massage, exercise, and manual therapy. These may help by improving circulation, muscle coordination, and immune response, though conclusive evidence is limited (Rapaport, Schettler, & Bresee, 2012). Recently, cervical stabilization exercises, especially those targeting the craniocervical flexor (CCF) muscles, have gained attention for improving posture and reducing pain (Jull, Kristjansson, & Dall’Alba, 2004). Techniques like CCF exercises, manual therapy, and specific stretching have shown promising results (Dunning et al., 2012).
However, most treatments rely on therapists, and few studies combine cervical movement and exercise or focus on young adults. There is also a lack of long-term randomized clinical trials on this topic. This study aims to demonstrate the effectiveness of cervical movement and stabilization exercises for managing chronic neck pain in adults.
2. Materials and Methods
2.1. Participants
The study participants were members of private training centers in Seoul, South Korea. Among the participants who agreed to be included in this study, 45 were selected based on inclusion and exclusion criteria. Inclusion criteria were as follows: young men and women who have complaints of neck pain with a neck disability index (NDI) of 15–24 points corresponding to moderate disability (Vernon & Mior, 1991). Exclusion criteria were as follows: individuals with 1) a history of neck and/or shoulder surgery including disk prolapse and cervical stenosis, 2) a history of severe trauma (such as neck pain and structural deformation), 3) rheumatism, 4) tumor, or 5) osteoporosis. 45 people participated in the study and 4 people dropped out; thus, data of 41 participants were finally analyzed. Given the differential and synergistic effects of mobilization, exercise, and stretching reported in previous studies, dividing participants into three groups allows for a valid comparison of their therapeutic outcomes in managing chronic non-specific neck pain. Therefore, participants in this study were randomly assigned to three groups: Accordingly, a randomized allocation was used to assign participants to one of the three groups: MES (Mobilization, Exercise, and Stretching, n=15), ES (Exercise and Stretching, n=15), and St (Stretching, n=15) (Kocaman, Yıldız, Canlı, & Alkan, 2023; Rodríguez-Sanz et al., 2021; Ylinen et al., 2003). This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (1044308-202201-HR-001-01). The researcher explained the purpose of the study to all participants, and they signed a consent form to participate in this study.
2.2. Cervical Spine Mobilization program
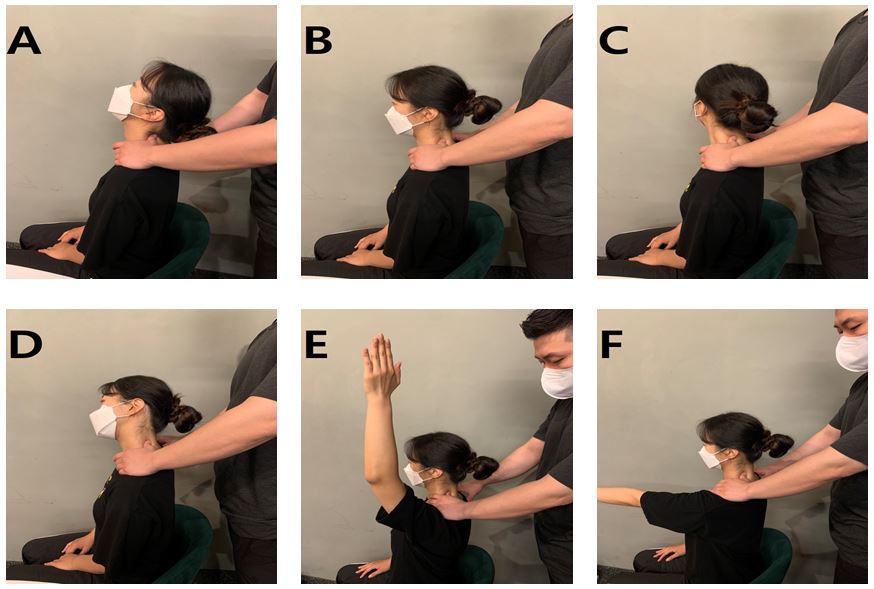
Participants performed a cervical spine mobilization program 3 times per day for 12 weeks. Based on previous research, the program targeted deep cervical muscles and joint movement (Buyukturan, Buyukturan, Sas, Karartı, & Ceylan, 2018). Movements followed a specific order (Figure 1A–F) and were guided by a certified therapist with over 10 years of experience. If symptoms like radiating pain or paralysis occurred, the session was stopped and safety measures were taken. Checking the cervical segments (C1–C7) and providing pressure to the transverse process where discomfort was observed, along with gradually increasing range of motion for comfort, were all part of mobilization.
2.3. Cervical stabilization movement program
Participants performed the stabilization exercise program daily for 12 weeks, with each session repeated three times (Buyukturan et al., 2018). The MES and ES groups performed exercise and stretching together. The program, based on prior studies, targeted deep cervical muscles and spinal alignment (Durall, 2012; Hoy, Protani, De, & Buchbinder, 2010). Exercises were performed in a specific sequence (Figure 2A–E), with stretching before and a 5-minute cool-down after.
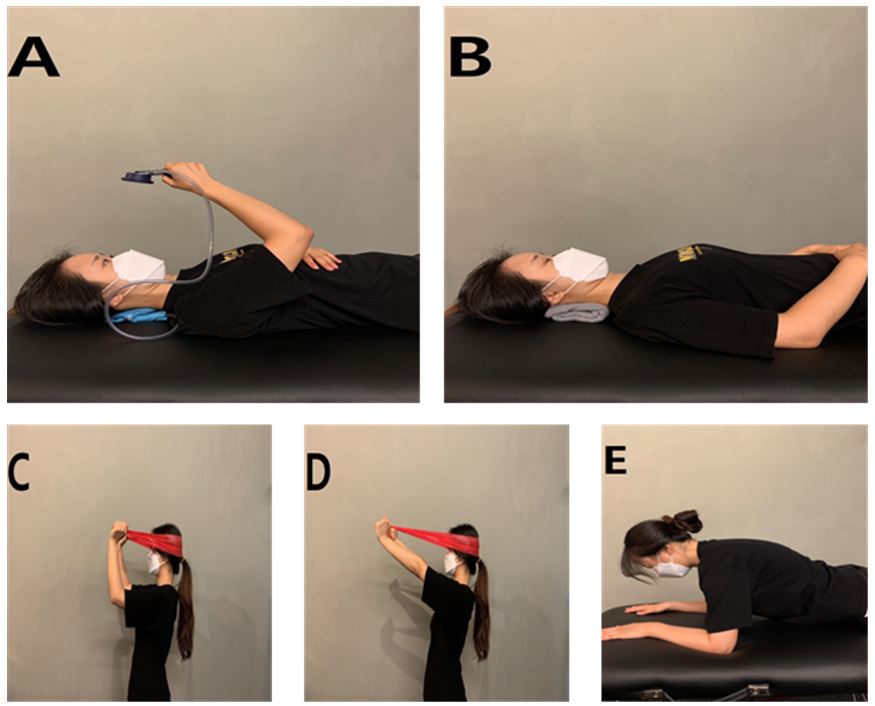
In the supine position, a pressure biofeedback device was placed between C1–C7. Participants gently pulled the chin to raise pressure from 20‒40 mmHg, avoiding overuse of the sternocleidomastoid. Exercises continued with towel support (Figure 2B), resistance band training (Figures 2C–D), and prone trunk extension while maintaining spinal alignment (Figure 2E). Sessions were halted if radiating pain or paralysis occurred, following safety protocols.
Table 1.
Mobilization and Stabilization exercise program
| Programs | Intervention | Duration | Repeat | Number of days |
| Mobilization program | Before the intervention, touch the transverse protrusion of the subject and check the range of motion and pain through the movement of the cervical vertebrae (C1 to C7). | 20 min | 3 times | 7 |
| Figures 1A and B show cervical elongation and flexion; sitting, touching the transverse projections in order of the upper and lower cervical vertebrae, and moving the neck up and down. | ||||
| In Figure 1C, turn the cervical vertebrae; sit down, touch the transverse projection in the order of the upper and lower cervical vertebrae, and move the neck left and right. | ||||
| In Figure 1D, lateral flexion of the cervical vertebrae; sit down, touch the transverse projection in order of the upper and lower cervical vertebrae, and tilt the neck left and right. | ||||
| Figures 1E and F show the extension and flexion of the arm; sitting, touching the transverse projection in the order of the upper and lower cervical vertebrae, and move the arm from top to bottom, from outside to inside. | ||||
| After the intervention, the subject takes a deep breath in an angst position and relaxes from the tense state. | ||||
| Stabilization exercise | From the beginning to the fourth week, as shown in Figure 2A below, pull the chin with the stabilizer on the back of the neck while lying down, and pull the chin with the towel on the back of the neck while lying down as shown in Figure 2B. | |||
| Figure 2C and D show the band at the back of the head and the pull of the chin to push the head back while sitting, including the above program from week 5 to week 8. | ||||
| Figure 2E includes a program from week 9 to week 12 that puts your hands and elbows on the floor while lying on your stomach, pulling your chin, and pushing your neck back. | ||||
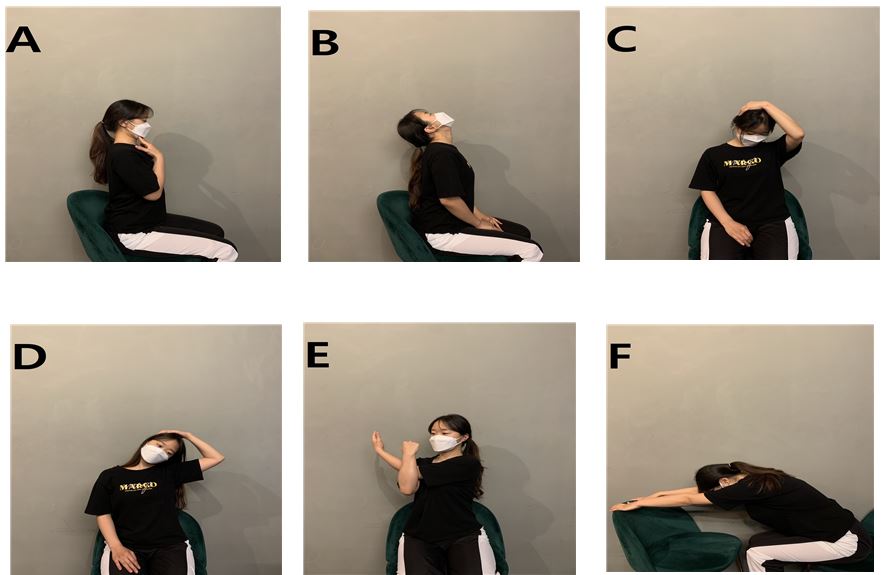
| Stretching exercise | Figure 3A Sit on the chair and pull your chin. | |||
| Figure 3B Sit on a chair and tilt your head back. | ||||
| Figure 3C Sit on a chair and hold your head at a 45° angle and press it. | ||||
| Figure 3D Sit on a chair, tilt your neck to the side, hold your head, and press it. | ||||
| Figure 3E Sit on the chair and stretch your shoulder by pressing your elbow with one arm. | ||||
| Figure 3F Sit on the chair and stretch your arms forward. |
2.4. Stretching exercise program
Participants performed the stretching program daily for 12 weeks, repeating each session three times per day (Monticone et al., 2012). All groups participated together. The program, based on previous studies, focused on stretching deep cervical and shoulder muscles prone to tension (Noormohammadpour, Tayyebi, Mansournia, Sharafi, & Kordi, 2017). Exercises followed a set sequence (Figure 3A–F), and were stopped immediately if radiating pain or paralysis occurred.
The method involved seated postures with the back straight and chin tucked (Figure 3A), followed by slow head tilts backward and sideways without raising the jaw (Figures 3B–D). Gentle hand-assisted diagonal and lateral stretches were held for 3 seconds if pain was felt. Additional stretches included arm positioning for muscle relaxation (Figures 3E–F), ensuring a gradual and safe range of motion.
2.5. Mesurements
2.5.1 Visual analog scale (VAS)
VAS was used to evaluate the participant’s neck pain level. The VAS used was a 10-cm line with a scale of 0 to 10 and with anchor statements on the left (no pain) and on the right (deathly pain). As a measure of pain, the participants directly marked their level of pain on the 10-cm horizontal line (Scott & Huskisson, 1979).
2.5.2 Neck Disability Index (NDI)
The degree of neck dysfunction was evaluated by Korean version of the NDI (0–50 points score; the higher the score, the higher the functional disorder). The intra-class correlation coefficient (ICC) of the tool's reliability test-retest is 0.82 and Cronbach's α is 0.93 (Song, Choi, Choi, & Seo, 2010).
2.5.3 Cervical range of motion (CROM)
CROM (Performance Atonement Associates, St Paul, MN, USA) cervical spine angular meter was used to measure the range of joint motion of the cervical spine. The CROM consists of three inclinators, and after wearing glasses on the face, it is fixed with an adhesive Velcro at the back of the head. The two inclinators on the side of the head and on the forehead are gravity-based inclinators for measuring elongation, flexion, and external flexion, and the other is a magnetic inclinometer that can measure the rotation of the head only for a magnet fixed to the upper body to exclude movement between bodies (Rheault et al., 1992). The range of neck joint motion of the participant’s extension, flexion, left lateral flexion, right lateral flexion, left rotation, and right rotation was measured. In the study of the reliability was Cronbach's α = 0.92.
2.5.4 Stabilizer pressure biofeedback
In order to measure the muscle strength and muscle endurance of the cervical spine, 50% of maximum muscle strength (MMS) and 50% of MMS time were calculated using a stabilizer pressure biofeedback muscle testing device (Chattanooga Inc., Chattanooga, TN, USA). We installed the pressure biofeedback equipment in the lower cervical space facing the ceiling and ensuring that the participant’s head was naturally maintained while lying down. To reduce the space between the cervical spine and the equipment as much as possible, the pressure was started at 20 mmHg and increased by 2 mmHg up to 40 mmHg in consideration of the participant’s physical characteristics (Chiu, Hui-Chan, & Cheing, 2005). The experimenter measured the MMS (mmHg) when pulling the chin without raising the head, and in the case of 50% MMS time, the time to maintain based on the 50% pressure of MMS was recorded in seconds. When measuring the MMS, a rest time of 1 minute was provided between measurements, and the largest value was selected from a total of 5 measurements. Furthermore, 50% MMS time was measured with a rest time of 5 minutes before measurement; when an error of 2 mmHg occurred in 50% MMS time between measurements, measurement was stopped and the time was recorded.
2.6. Statistical analysis
Using G-power 3.1.9.4 version (Heinrich-Heine-Universität, Düsseldorf, Germany), repeated measurement variance analysis, two-sided test, moderate effect size = 0.25, significance level = 0.05, power = 0.9, and repeated measurement of three times, the required appropriate sample size was calculated to be 39 (Cohen, 2013).
The means and standard deviations (SDs) were computed for each main dependent variable. The general characteristics among groups were analyzed by the one-way ANOVA (analysis of variance) test for continuous variables, the corresponding sample t-test for before and after the group, the repeated two-way ANOVA was used, and the difference between groups was tested with Tukey honestly significant difference (HSD). The Statistical Package for Social Science was used (SPSS, version 25.0, IBM Corp., Armonk, NY, USA). The statistical significance level was set to p < .05.
3. Results
3.1. Subjects
As shown in Table 2, the physical characteristics of the participants did not differ significantly among groups (p > .05).
Table 2.
Characteristics of participants in groups
3.2. Changes in the range of neck joint movement
A two-way repeated measures ANOVA (3 groups × 2 time points) and a one-way ANOVA were conducted to examine of the MES, ES, and St exercise programs. The results are presented in Table 3.
Table 3.
Changes in the cervical range of motion
Values are expressed as mean ± standard deviation. MESa: mobilization, exercise, and stretching intervention group; ESb: exercise and stretching intervention group; Stc: stretching intervention group; †Significant difference from pre-intervention, p < 0.05; *significant difference by two-way ANOVA, p < 0.05; abc: Tukey post-hoc test.
A significant group × time interaction effect was observed for cervical spine range of motion (ROM) in flexion (p < .001), extension (p < .001), right lateral flexion (p < .012), left lateral flexion (p < .002), right rotation (p < .001), and left rotation (p < .009). Post-hoc analysis revealed that flexion, extension, right rotation, and left rotation improved in the order of MES , ES, St. For right and left lateral flexion, the MES group showed significantly greater improvements in ROM compared to the ES and St groups.
All three groups showed significant improvements in cervical ROM following the intervention compared to baseline. However, in the St group, improvements in extension (p < .136) and left rotation (p < .212) were not statistically significant.
3.3. Change in muscle functions
A two-way repeated measures ANOVA (3 groups × 2 time points) and a one-way ANOVA were conducted to examine of the MES, ES, and St exercise programs. The results are presented in Table 4. A significant group × time interaction effect was observed for both muscle strength (p < .001) and muscle endurance (p < .001). Post-hoc analysis revealed that the MES group showed significantly greater improvements in both muscle strength and endurance compared to the ES and St groups. All three groups showed significant enhancements in muscle strength (p < .001) and muscle endurance (p < .001) following the intervention compared to baseline. However, in the St group, increase in muscle strength was not statistically significant.
Table 4.
Changes in Muscle Functions
3.4. Changes in the neck pain VAS and NDI
A two-way repeated measures ANOVA (3 groups × 2 time points) and a one-way ANOVA were conducted to examine of the MES, ES, and St exercise programs. The results are presented in Table 5. A significant group × time interaction effect was observed for VAS (p < .001) and NDI (p < .001) score. Post-hoc analysis revealed that the MES group showed significantly greater reductions in both VAS and NDI compared to the ES and St groups. All three groups showed significant reductions in VAS and NDI scores following the intervention (p < .001), indicating improvements in pain and neck disability.
Table 5.
Changes in neck pain
Values are expressed as mean ± standard deviation. MESa: mobilization, exercise, and stretching intervention group; ESb: exercise and stretching intervention group; Stc: stretching intervention group; †Significant difference from pre-intervention, p < 0.05; *significant difference by two-way ANOVA, p < 0.05; abc: Tukey post-hoc test.
4. Discussion
With the widespread use of computers and smartphones—especially heightened during the Coronavirus disease 2019 (COVID-19) pandemic—neck pain has become increasingly common due to neck fatigue and mechanical stress. This study evaluated the effects of cervical movement, stabilization exercises, and stretching on neck mobility, strength, endurance, pain, and disability.
Results showed significant improvements in cervical flexion, extension, and rotation across all groups. However, right and left flexion showed group-specific differences: right flexion was significantly different only between MES and ES groups, while left flexion differed significantly between MES and St groups. These findings suggest that the combination of mobilization, exercise, and stretching may provide additional benefits in improving specific directional movements of the cervical spine that are less responsive to stretching or exercise alone. Except for extension and left rotation in the St group, all other parameters showed significant pre-post improvements in the MES and ES groups. This supports the view that active intervention involving movement and stabilization is more effective than passive stretching alone in enhancing cervical function.
In previous studies, stabilization exercise and hand therapy were reported to be effective in improving cervical range(Kay et al., 2012); application of cervical spinal manual therapy to 105 neck pain patients was reported to result in an 8‒12% increase in joint range in all six domains of neck range (curving, kidney, lateral flexion, and axial flexion)(Celenay, Akbayrak, & Kaya, 2016). Consistent with these findings, the present study also observed improvements in cervical range of motion across all groups, with post-intervention gains of 9.66° in the MES group, 5.6° in the ES group, and 0.74° in the St group. Similarly, Neumann et al. reported post-intervention improvements of 7.8°, 4.53°, and 1° in the MES, ES, and St groups, respectively, compared to a pre-defined maximum operating range of 40°, while Whittingham & Nilsson (2001) found right-side motion improvements of 4.86° in the MES group and 3.07° in the ES group. Taken together, these prior and current results reinforce the view that cervical mobilization combined with exercise and stretching is more effective than exercise or stretching alone in restoring functional joint mobility.
Regarding muscle endurance, there were significant differences between the three groups. Post-hoc analysis showed that all intergroup comparisons (MES vs. St, MES vs. ES, ES vs. St) were significant. The pre- and post-intervention changes in muscle endurance were also significant within all groups. This suggests that even stretching alone may contribute to endurance gains, but the additive effect of mobilization and exercise results in substantially greater improvements.
According to a previous report (Tsakitzidis, Remmen, Dankaerts, & Van Royen, 2013), cervical movement and stabilization exercise showed improvement in muscle and muscle endurance ability; the results of this study also show that a MES approach produces superior outcomes across strength, endurance, and mobility domains compared to ES and St approaches. Additionally, Neumann (2002) reported that cervical stabilization stimulation can trigger mechanoreceptors that activate descending pain inhibition pathways, thereby reducing pain and muscle guarding. This neurophysiological mechanism may partially explain the pain-reducing effects observed in the MES group, supporting the hypothesis that targeted movement and neuromuscular control exercises can influence central pain modulation.
Changes in neck pain intensity showed significant differences among the MES, ES, and St groups. Post-hoc analysis revealed significant reductions in the MES vs. St and MES vs. ES comparisons, but not between ES and St. This finding reinforces the superiority of including mobilization in treatment protocols to achieve meaningful pain relief.
NDI (Neck Disability Index) scores showed significant intergroup and intragroup changes. The MES group showed the largest reduction, followed by the ES group. Although all groups improved, the significantly greater reduction in disability in the MES group may reflect the comprehensive nature of the intervention, addressing both biomechanical and neuromuscular dysfunctions.
NDI scores showed significant intergroup and intragroup changes. The MES group showed the largest reduction, followed by the ES group. Although all groups improved, the significantly greater reduction in disability in the MES group may reflect the comprehensive nature of the intervention, addressing both biomechanical and neuromuscular dysfunctions.
Previous studies have reported a 22% reduction in NDI among women receiving hand therapy and stabilization exercises (Kay et al., 2012; Walker et al., 2008), and improvements in disability with combined manual therapy and exercise (Falla, Lindstrøm, Rechter, Boudreau, & Petzke, 2013). Consequently, the effects of poor posture on cervical joints, muscles, and adjacent tissues were improved through cervical movement, stabilization, and stretching. Moreover, enhanced vascular perfusion to cervical arteries—potentially stimulated through mobilization—may have contributed to improved tissue health and joint mobility. This study confirmed that cervical movement, stabilization exercise, and stretching can improve the range of neck joint movement, muscle strength, muscle endurance, pain, and NDI in adults with chronic non-specific neck pain. Importantly, the results suggest that an integrated, MES exercise protocol is more effective than Es and St interventions, underscoring the value of combined strategies in conservative neck pain management.
5. Conclusion
This study demonstrates that while stretching and exercise independently offer therapeutic benefits for managing chronic non-specific neck pain in young adults, the combination of mobilization, exercise, and stretching (MES) yields superior outcomes in pain reduction and functional improvement. These findings suggest that an integrated intervention approach may be more effective than conventional single-modality strategies, and should be considered in the design of neck pain management programs for this population.
