

1. Introduction
2. Methods
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
2.3. Study Selection
2.4. Charting the Data
3. Results
3.1. Collating, Summarizing, and Reporting the Results
4. Discussion
5. Conclusions
1. Introduction
Globally, healthcare systems are facing mounting challenges due to declining birth rates and an aging population. These demographic shifts have led to a growing burden of care and a significant shortage of healthcare personnel, including care workers, nurses, and therapist (Cresswell, Callaghan, Mozaffar, & Sheikh, 2019; Tetsuya, 2017). Addressing this issue requires innovative approaches to enhance the efficiency and sustainability of healthcare services. One promising solution is the development and adoption of care robots, which have gained attention for their potential to reduce the physical demands on caregivers and support the independence of elderly or disabled individuals. Governments and industries are increasingly investing in care robot research, anticipating improvements in service delivery and opportunities for industrial innovation (Kim, Park, & Ryu, 2022; Lee et al., 2018)
According to ISO 8373:2021, robots are defined as programmed mechanisms capable of autonomous or semi-autonomous physical tasks (Teng, Ding, & See, 2022). Care robots, specifically, are designed to support the physical, cognitive, and emotional needs of both care recipients and healthcare providers (Goeldner, Herstatt, & Tietze, 2015; Glende, Conrad, Krezdorn, Klemcke, & Krätzel, 2016). These robots can perform repetitive or strenuous tasks, thereby reducing caregiver workload, improving care quality, and enhancing the safety and quality of life for patients. Research has shown that care robots can positively influence clinical outcomes, such as mobility, satisfaction, and even mortality rates among older adults (Teng et al., 2022; Kulich, Wei, Crytzer, Cooper, & Koontz, 2021). They also contribute to increased job satisfaction among healthcare professionals (Lee et al., 2018).
Despite these benefits, there are notable concerns and barriers to implementation. Ethical and legal challenges, such as privacy violations, reduced autonomy, and social isolation, must be addressed (Teng et al., 2022; Johansson-Pajala & Gustafsson, 2022). Financial limitations, negative public perceptions, and potential disruptions to existing workflows further hinder the integration of care robots into healthcare systems. Thus, a balanced understanding of both the advantages and the limitations of care robots is necessary.
To explore this complex issue, this study adopts a sociotechnical framework, which emphasizes the reciprocal relationship between technological innovations and the social environment. From this perspective, care robot development is shaped by societal needs and cultural values, while their introduction reshapes professional roles and care processes (Cresswell, Callaghan, Mozaffar, & Sheikh, 2019; Cresswell, Cunningham-Burley, & Sheikh, 2018). By applying this conceptual approach, the study aims to synthesize recent evidence on care robots and identify key factors that influence their effective implementation in healthcare settings.
2. Methods
2.1. Identifying the Research Question
A scoping review summarizes and evaluates research before a systematic review, mapping evidence types, data, and concepts to identify study differences and address diverse research questions within a specific topic. This scoping review aimed to comprehensively synthesize existing literature on the use of care robots in elderly care to achieve an integrated understanding of recent research, with particular emphasis on sociotechnical perspectives—specifically, the technical, social/human, organizational, and macroenvironmental dimensions. The review followed the methodological framework proposed by Arksey and O’Malley and adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) checklist to ensure transparency and methodological rigor.
The primary research question guiding this review was: What values, benefits, or barriers are associated with the application of care robots in healthcare services? This question directed the selection of relevant literature and the interpretation of the findings within a sociotechnical framework.
2.2. Identifying Relevant Studies
A comprehensive literature search was conducted to identify relevant peer -reviewed articles published between January 2018 and January 2023. The search was carried out across four major databases: PubMed, Embase, Cochrane Central, and CINAHL. Keywords included variations and combinations of terms such as “aged,” “elderly,” “robotics,” “caregiver,” “burnout,” “usability,” and “social values,” combined using Boolean operators “AND” and “OR.”
2.3. Study Selection
After removing duplicate entries, articles were screened for eligibility based on predefined inclusion and exclusion criteria. Studies were selected if they met the following inclusion criteria: (1) focused on elderly individuals, particularly those requiring physical support for daily activities such as bathing, feeding, or toileting; (2) involved healthcare personnel including care workers, nurses, and therapists; (3) investigated the use of care robots supporting physical functions in daily living; (4) discussed sociotechnical aspects, including labor implications, ethical issues, or technological innovation; and (5) were published in English.
Exclusion criteria included studies involving elderly individuals with cognitive or psychological impairments such as dementia or psychiatric conditions, studies focused solely on cognitive support, chatbots, AI-only technologies, or surgical/ diagnostic robots, and papers that did not provide full-text access (e.g., abstracts, posters, commentaries). Furthermore, studies focusing exclusively on technical innovation without human factors or interaction were excluded, as were those related to AR, VR, telemedicine, or deep learning technologies unrelated to physical caregiving.
2.4. Charting the Data
Relevant data were extracted and organized using Microsoft Excel. Data fields included study author(s), year of publication, country, study design, population, type of robotic intervention, and sociotechnical dimensions. Included study designs comprised literature and systematic reviews, mixed-methods studies, clinical trials, qualitative studies, and case studies.
Key stakeholders identified across the literature included direct care users (e.g., elderly individuals and those with neurological diseases such as Parkinson’s disease or stroke), formal caregivers (e.g., nurses and therapists), healthcare providers, robotic developers, and policymakers (Omachonu & Einspruch, 2010). Interventions focused on robot-assisted support either directly for older adults or indirectly for care providers, aiming to enhance care delivery and address labor challenges in long-term care.
Outcomes were thematically analyzed and classified based on Cresswell et al.’s sociotechnical framework (Cresswell et al., 2018). The technical dimension referred to studies evaluating usability and technological integration in real-world contexts. The social/human dimension included findings related to user satisfaction, engagement, resistance, training, and caregiver interaction. The organizational dimension covered themes such as institutional readiness, leadership, communication, and implementation strategies. Lastly, the macroenvironmental dimension addressed broader contextual factors, including political, economic, legal, and ethical considerations.
3. Results
3.1. Collating, Summarizing, and Reporting the Results
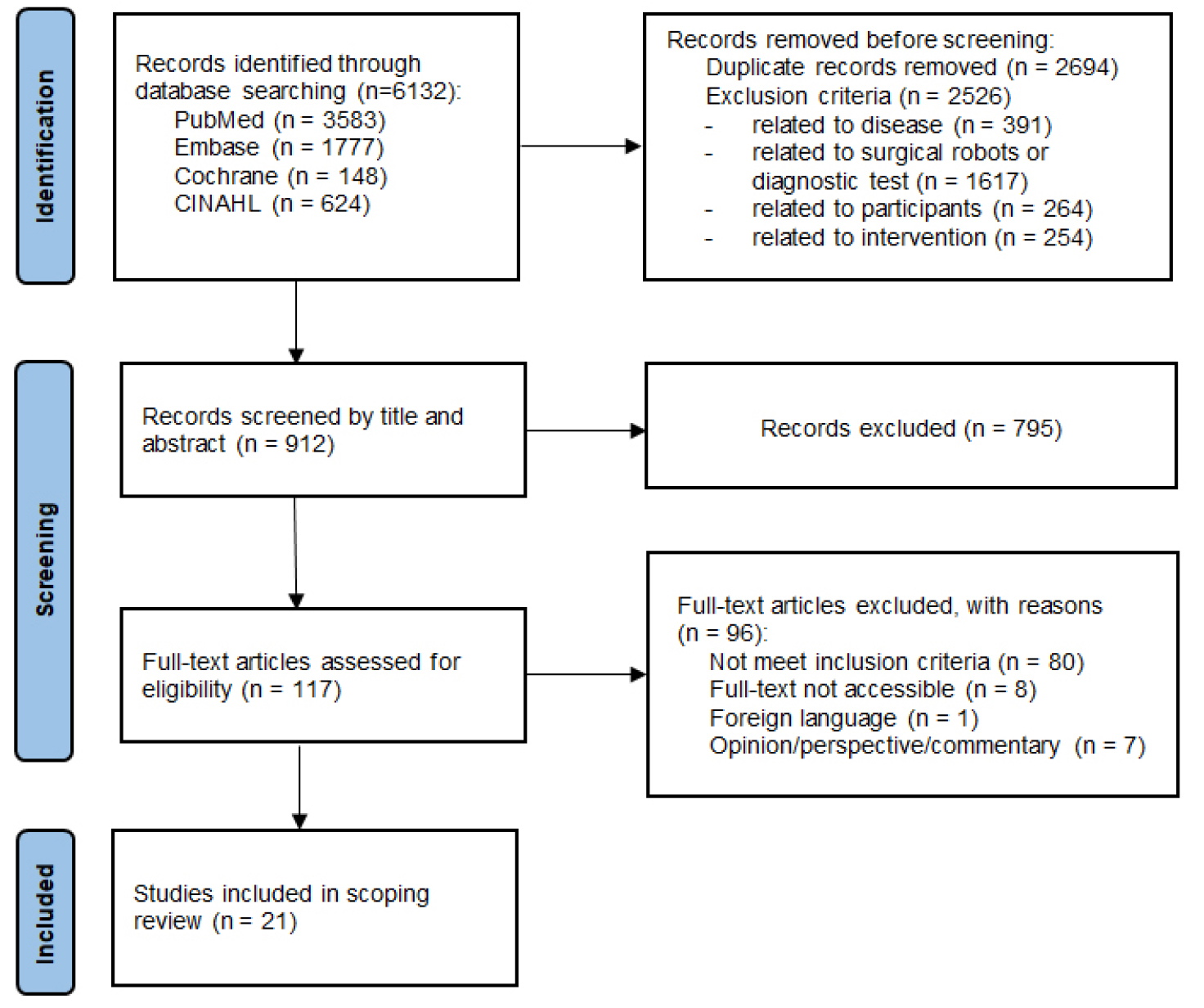
An initial total of 6,132 studies were retrieved. Following the removal of 5,220 duplicates and irrelevant articles based on title and abstract screening, 912 articles remained. Of these, 117 articles were selected for full-text review using the EndNote software. After a systematic assessment and consensus -building process among four independent reviewers, a final total of 21 studies were included in this scoping review (Figure 1).
3.1.1 Characteristics of the selected studies
21 selected studies are shown in Table 1. The selected studies varied in design and focus. By publication year, the majority were published in 2022 (33.3%), followed by 2018 (23.8%) and 2020 (19.0%). The studies were conducted in various countries, including European nations such as Germany, Italy, and the United Kingdom, as well as the United States, Japan, China, and South Korea. Literature and systematic reviews and trials were the most prevalent designs (each 28.6%), followed by mixed-methods research (19.0%), case studies (14.3%), and qualitative studies (9.5%).
With respect to participant focus, 11 studies (52.4%) centered on healthcare personnel, while 7 (33.3%) focused on elderly care recipients and 5 (23.8%) on informal caregivers. Additionally, 3 studies (14.3%) explored perspectives from diverse stakeholders, including engineers, technologists, strategists, and policy actors. In terms of intervention types, 7 studies (33.3%) addressed robot -assisted interventions, while 14 studies (66.7%) focused on supportive care robot systems.
3.1.2 The sociotechnical perspectives of care robots
The selected studies categorized sociotechnical perspectives on care robots into different dimensions: the technical dimension, the social/human dimension, the organizational dimension, and the macroenvironmental dimension.
The technical dimension of care robots was a consistent focus in 16 of 21 studies (76.2%), followed by the social/human dimension, on which 14 of 21 studies (66.7%) focused. Next, the organizational dimension was addressed by 10 studies (47.6%), and the macroenvironmental dimension was included in 5 studies (23.8%). Notably, five studies (23.8%) comprehensively incorporated insights from all four dimensions. The outcomes of the selected studies were identified within each of the four dimensions.
• Technical Dimension: Outcomes included technology acceptance, robot appearance, technological challenges, and differences between robot-assisted and conventional interventions.
• Social/Human Dimension: From the care recipients’ perspective, outcomes included health management functions, decreased mortality rates, and improvements in physical independence and psychosocial well-being. From the caregivers’ perspective, outcomes included the provision of fundamental care, improved safety, positive attitudes toward care recipients, enhanced care activity, and reduced perceived physical demands.
• Organizational Dimension: Outcomes included an altered scope of nursing practice, improved collaboration, the integration of mechanistic and relational care, reliable implementation, enhanced productivity, and cost savings.
• Macroenvironmental Dimension: Outcomes included social trust, the experience of autonomy, power structures, privacy concerns, data security, economic considerations, and ethical challenges related to robotic care.
Table 1.
Summary of Selected Studies
| Author, year | Country | Study design | Study population | Interventions | Sociotechnical perspective of care robots |
| Archibald et al., 2018 | Australia | Literature review | Health care personnel | Supportive Care Robot/ Robot System |
Social/human dimension Organizational dimension |
| Brinkmann et al., 2022 | Germany | Trial | Health care personnel | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension |
| Cresswell et al., 2018 | UK | Qualitative study |
Health care personnel Other stakeholders: engineers, technologists, academics, marketing, strategists, managers | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension Macroenvironmental dimension |
| D'Onofrio et al., 2018 | France, Italy, Netherlands, Japan | Mixed method research | Older adults Caregivers | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension |
| Fay et al., 2023 | Ireland | Trial | People with stroke and Parkinson’s disease | Robot-Assisted Intervention | Technical dimension |
| Franke et al., 2021 | Germany | Review | Health care personnel | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension Macroenvironmental dimension |
| Guo et al., 2022 | China | Trial | People with stroke | Robot-Assisted Intervention | Technical dimension |
| Jin et al., 2018 | China | Case study | Older adults | Robot-Assisted Intervention | Technical dimension |
| Johansson et al., 2022 | Sweden | Qualitative study |
Older adults Health care personnel Other stakeholders: business developers, marketing managers, strategists | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension Macroenvironmental dimension |
| Kadone et al., 2020 | Japan | Case study | People with dropped head syndrome | Robot-Assisted Intervention | Technical dimension |
| Kato et al., 2023 | Japan | Trial | Caregivers | Supportive Care Robot/ Robot System | Social/human dimension |
| Kim et al., 2022 | Republic of Korea | Mixed method research |
Older adults Caregivers Health care personnel | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension Macro-environmental dimension |
| Koseki et al., 2020 | Japan | Case study | Older adults | Robot-Assisted Intervention | Technical dimension |
| Kowalski et al., 2020 | Germany | Trial | Health care personnel | Supportive Care Robot/ Robot System | Social/human dimension |
| Laparidou et al., 2021 | UK | Mixed method research |
People with motor rehabilitation Caregivers, Health care personnel | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension |
| Martini et al., 2019 | Italy | RCT | Older adults | Robot-Assisted Intervention | Technical dimension |
| Mitzner et al., 2018 | USA | Mixed method research | Health care personnel | Supportive Care Robot/ Robot System |
Social/human dimension Organizational dimension |
| Mois et al., 2020 | USA | Review |
Older adults Caregivers Health care personnel Other stakeholders: managers, technologists, healthcare policy makers | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension Macro-environmental dimension |
| Sattelmayer et al., 2019 | Switzerland |
Systematic review Meta-regression | People with multiple sclerosis | Robot-Assisted Intervention | Technical dimension |
| Teng et al., 2022 | Singapore | Systematic review | Patients in critical care | Supportive Care Robot/ Robot System |
Social/human dimension Organizational dimension |
| Zanatta et al., 2022 | Italy | Systematic review | People with stroke and Parkinson’s disease Health care personnel | Supportive Care Robot/ Robot System |
Technical dimension Social/human dimension Organizational dimension |
4. Discussion
This scoping review examined the sociotechnical dimensions of care robots used in elderly care, categorizing the findings into four key domains: technical, social/human, organizational, and macroenvironmental.
Technical Dimension: User acceptance emerged as a critical theme within the technical dimension. Several studies emphasized that care robots will be more readily accepted if their design reflects the needs and capabilities of end users—particularly elderly care recipients with physical or cognitive impairments (Zanatta, Giardini, Pierobon, D'Addario, & Steca, 2022; Franke, Nass, Piereth, Zettl, & Heidl, 2021). Environmental factors also influence robot usability; for instance, physical barriers such as narrow doorways or uneven flooring can limit robot functionality (Cresswell et al., 2019). These findings underscore the necessity of fostering collaboration between developers, end users, and care institutions during the design and testing phases (Laparidou et al., 2021).
Recent literature has also highlighted the concept of co-creation, wherein end users—elderly individuals, caregivers, and other stakeholders—are engaged in the development process through interviews and participatory design sessions (Soriano et al., 2022). This approach ensures that care robots align with user expectations, leading to improved acceptance and functionality in real-world settings. Technological innovation, in this context, must be deeply interwoven with human-centered care practices to avoid depersonalization and reinforce dignity.
Social/Human Dimension: Care robots demonstrated the potential to enhance physical independence and psychosocial well-being among care recipients, as well as to reduce the physical burden on caregivers (Kowalski, Arizpe-Gomez, Fifelski, Brinkmann, & Hein, 2020). However, ethical concerns persist regarding the potential dehumanization of care, the objectification of care recipients, and job insecurity among caregivers (Mois & Beer, 2020; Archibald & Barnard, 2018; Carter-Templeton, Frazier, & Wyatt, 2018). These concerns reflect a broader debate: while care robots are promising for tasks that are physically strenuous—such as lifting or transporting patients—they remain limited in their ability to provide emotionally intelligent care (Bedaf, Marti, Amirabdollahian, & de Witte, 2018).
Notably, studies have shown that caregivers find robots most useful for physically demanding tasks. For example, humanoid robots were viewed as effective in handling aggressive patients and improving safety in high-risk care environments (Carter-Templeton et al., 2018). This suggests that the optimal role for care robots may lie in supplementing human labor in tasks that are physically taxing or dangerous, rather than in providing psychological or emotional support.
Organizational Dimension: The integration of care robots into healthcare settings requires careful consideration of the organizational dimension, particularly in redefining roles and responsibilities. Studies suggest that adjusting the scope of practice and developing an appropriate skill mix between human caregivers and robots can address workforce shortages in eldercare (Tetsuya, 2017; Lee et al., 2018; Archibald & Barnard, 2018; Soriano et al., 2022). When robots are tasked with repetitive and time-consuming activities—such as feeding, bathing, or toileting—human caregivers can focus on delivering relational and emotional care, thereby improving both efficiency and care quality (Kim et al., 2022).
This complementary division of labor supports the concept of slow nursing care, which emphasizes unhurried, person -centered care. Robots enable patients, especially those with dementia, to complete daily tasks at their own pace, while caregivers gain more time to build therapeutic relationships (Lillekroken, 2015).
Additionally, deploying different types of robots tailored to specific functions can further enhance care delivery when integrated effectively into care teams (Kim et al., 2022; Archibald & Barnard, 2018; Mitzner, Tiberio, Kemp, & Rogers, 2018).
While robots may be well-suited for cognitive or mechanistic tasks, human caregivers remain essential for emotional care and therapeutic touch—elements that reinforce dignity, comfort, and human connection (Wang & Krumhuber, 2018). This interdependence leads to the concept of triadic care, involving collaboration between the caregiver, robot, and care recipient (Tetsuya, 2017). However, implementing this model raises concerns about task delegation, ethical boundaries, and maintaining care quality, indicating a need for continued research and ethical guidance in practice.
Macroenvironmental Dimension: The ethical, legal, and policy implications of care robot integration form a crucial aspect of the sociotechnical perspective. Key ethical concerns include the protection of privacy, autonomy, informed consent, and dignity—especially in light of risks related to surveillance, data misuse, and emotional isolation (Johansson-Pajala & Gustafsson, 2022). Public acceptance of care robots is also shaped by media portrayals, cultural perceptions, and the transparency of regulatory systems.
To promote ethical use, comprehensive national-level frameworks are required. These should encompass legislation, safety standards, data protection policies, and equitable funding mechanisms that ensure fair access to robotic technologies (Johansson-Pajala & Gustafsson, 2022). Equally important is the development of education and training programs for both caregivers and care recipients, which can improve understanding, increase acceptance, and reduce misuse (Zanatta et al., 2022; Sarbadhikari & Pradhan, 2020).
In addition, strategies to reduce implementation costs and adapt robot functions to population-specific risks and care needs are necessary (Kim et al., 2022). Ethical training should include real-world case studies, methods for early risk identification, and harm-reduction practices to support responsible and human-centered care robot use (Zanatta et al., 2022; Sarbadhikari & Pradhan, 2020).
This review has limitations, including the lack of formal quality assessment, exclusion of studies on cognitive or lab -based robotic functions, and restriction to recent publications. Consequently, foundational studies were omitted, and reliance on secondary sources may have limited the depth and comprehensiveness of primary evidence synthesis.
5. Conclusions
This study highlighted the sociotechnical perspective of care robots across four dimensions. Effective integration of care robots requires adjusting the scope of practice, skill mix, and task delegation between human caregivers and robots. Robots can assist with physical tasks like feeding and bathing, allowing human caregivers to focus on emotional care. This collaboration helps address the shortage of skilled workers. Additionally, successful implementation depends on cooperation with engineers, supportive environments, ethical standards, and team-based care models. These elements are essential for the sustainable and human-centered use of care robots in healthcare. Care robots show technical, social, and organizational benefits but face macro-level ethical, privacy, and trust barriers. Future research should integrate multidimensional perspectives for balanced adoption.
